Multiple Pathways to Recovery
A Research-Based Analysis of Secular and Higher Power-Based Recovery Models
An examination of the evidence base, clinical outcomes, and structural differences between spiritual and secular approaches to overcoming substance and maladaptive behaviors—and what the research means for individuals, clinicians, and policymakers.
Published by Amanda Scott-Telford for Emerging Whole • emergingwhole.org
February 2026
Executive Summary
Recovery from substance and maladaptive behaviors has historically been dominated by a single paradigm: the 12-step model, which centers on spiritual surrender and acknowledgment of powerlessness over one’s behavior. This model has provided meaningful support for millions of individuals worldwide. However, a growing body of peer-reviewed research demonstrates that secular, evidence-based recovery approaches produce comparable—and in some cases, superior—outcomes on key measures including total days abstinent, drinking intensity, mental health stability, and participant satisfaction.
This white paper synthesizes findings from major systematic reviews, randomized controlled trials, and comparative studies to provide an objective analysis of both recovery paradigms. Its purpose is not to advocate for one model over another, but to address a critical gap in public understanding: the research supports multiple pathways to sustained recovery, and the dominance of a single model in treatment referrals, court mandates, and public awareness may be leaving a significant portion of the recovery-seeking population underserved.
The evidence presented here has implications for clinicians making referral decisions, policymakers shaping treatment access, and individuals seeking a recovery path that aligns with their beliefs, needs, and goals.
1. The Problem: A One-Model Recovery System
Substance and behavioral health treatment in the United States has long been structured around the 12-step paradigm. A significant majority of inpatient and outpatient treatment programs incorporate 12-step principles, and court-mandated recovery frequently defaults to 12-step meeting attendance. While this model has a long track record of supporting recovery, its dominance creates a structural problem: individuals who do not connect with the spiritual framework of 12-step programs may disengage from recovery support entirely.
Data supports this concern. Research indicates that over 40% of individuals in recovery who identified as non-religious or uncertain about religion did not participate in 12-step meetings (Arista Recovery, 2025). This is not a marginal population. The Pew Research Center consistently finds that roughly 30% of U.S. adults identify as religiously unaffiliated—a share that has grown steadily over the past two decades. For these individuals, a recovery model built around surrender to a higher power may create a fundamental misalignment between the support being offered and the belief system of the person receiving it.
The issue is compounded by limited awareness. Many people seeking help for substance or maladaptive behaviors are never informed that secular, evidence-based alternatives exist. This is not because the alternatives lack research support, but because they lack the institutional visibility, meeting density, and cultural ubiquity of 12-step programming.
The Core Problem
When a single recovery model dominates treatment referrals and public awareness, individuals whose beliefs, needs, or clinical profiles do not align with that model are at increased risk of disengagement, treatment dropout, and relapse—not because recovery itself has failed them, but because the available framework has.
2. Higher Power-Based Recovery Models: Evidence and Limitations
2.1 Overview and Structure
The 12-step model, originating with the founding of Alcoholics Anonymous in the 1930s, follows a structured, sequential process that guides participants through admission of powerlessness over their substance or behavior, surrender to a higher power, moral self-inventory, amends-making, and ongoing spiritual maintenance. The model’s reach is substantial: it operates in over 180 countries, and related programs (Narcotics Anonymous, Gamblers Anonymous, and others) have extended its framework to a broad range of behavioral concerns.
2.2 The 2020 Cochrane Review: Key Findings
The most rigorous evaluation of 12-step effectiveness to date is the 2020 Cochrane Systematic Review conducted by Kelly, Humphreys, and Ferri. This review analyzed 27 studies encompassing 10,565 participants and compared Alcoholics Anonymous (AA) and clinically delivered Twelve-Step Facilitation (TSF) programs against other clinical interventions, including cognitive behavioral therapy (CBT) and motivational enhancement therapy (MET).
The review’s central findings were as follows:
Continuous abstinence. Manualized TSF programs produced higher rates of continuous abstinence at 12 months compared to other treatments (RR 1.21, 95% CI 1.03–1.42). This advantage was maintained at 24 and 36 months. The evidence suggested that approximately 42% of TSF participants remained completely abstinent at one year, compared to 35% in other treatment conditions (Kelly et al., 2020).
Other drinking outcomes. On measures of drinking intensity, percentage of heavy drinking days, and total days abstinent, AA/TSF performed comparably to other clinical treatments—showing no statistically significant advantage (Kelly et al., 2020).
Cost-effectiveness. Four of five economic analyses found substantial healthcare cost savings associated with AA/TSF, likely attributable to AA’s free, peer-led model reducing reliance on professional treatment services (Kelly et al., 2020).
2.3 Critical Methodological Considerations
While the 2020 Cochrane findings were widely reported as a definitive endorsement of the 12-step model, several methodological and interpretive nuances warrant close examination:
The continuous abstinence metric. The primary outcome favoring 12-step models—continuous abstinence—defines any substance use during the measurement period as total failure, regardless of overall trajectory. Heather (2021), in a peer-reviewed response published in Alcohol and Alcoholism, noted that this advantage did not translate into measurably less drinking frequency, intensity, or alcohol-related harm compared to other treatment conditions. The review also included no indices of quality of life or psychological well-being—measures now widely considered central to treatment evaluation.
The manualized vs. real-world gap. The strongest findings applied to clinically delivered, manualized TSF programs administered by trained counselors in controlled settings. This does not represent the typical 12-step experience, where most participants work the steps with an untrained peer sponsor rather than following a manualized clinical protocol (Practical Recovery, 2023). Of the 27 included studies, 24 were conducted in the United States, raising additional questions about generalizability (Heather, 2021).
The shift from the 2006 Cochrane Review. The earlier 2006 Cochrane Review of this topic, which employed broader outcome measures including quality of life and reduced dependence, reached a starkly different conclusion: “No experimental studies unequivocally demonstrated the effectiveness of AA or TSF approaches for reducing alcohol dependence or problems” (Ferri et al., 2006). The contrasting conclusions reflect, in significant part, which outcome measures were prioritized—a methodological choice, not a settled scientific fact.
Exclusion of mandated populations. The 2020 Cochrane Review explicitly excluded studies involving court-mandated or coerced participants. This means the positive findings for AA/TSF cannot be extrapolated to mandated treatment contexts—a common setting in which 12-step attendance is required.
3. Secular, Evidence-Based Recovery Models: Evidence and Outcomes
3.1 Overview and Principles
Secular recovery programs emerged in the 1970s and 1980s as structured alternatives for individuals who sought support without a spiritual or religious framework. Major programs include SMART Recovery (Self-Management and Recovery Training), LifeRing Secular Recovery, Secular Organizations for Sobriety (SOS), and Women for Sobriety. These programs share several core principles:
Self-empowerment over powerlessness. Rather than beginning from an admission of powerlessness, secular models frame recovery as the development of personal capacity—the ability to recognize patterns, regulate emotions, and make deliberate choices using learned skills.
Evidence-based therapeutic tools. These programs draw from established therapeutic modalities including cognitive behavioral therapy (CBT), Rational Emotive Behavior Therapy (REBT), motivational interviewing, and applied neuroscience. Participants learn specific, replicable strategies such as cognitive restructuring, cost-benefit analysis for urges, the ABC-DE method for examining irrational beliefs, and behavioral activation techniques.
Individualized, non-prescriptive structure. Rather than a fixed sequence of steps, secular programs provide a toolkit from which individuals can draw based on their specific needs, co-occurring conditions, and personal goals.
Secular inclusivity. By removing the requirement of belief in a higher power, these programs provide a recovery pathway accessible regardless of religious identity, spiritual orientation, or lack thereof.
3.2 Research Findings
Comparable abstinence rates. Research published in the Journal of Substance Abuse Treatment found that participants in secular recovery programs achieved similar rates of abstinence and overall improvement compared to 12-step participants. The study also identified higher satisfaction rates among participants who identified as atheist or agnostic—a finding with significant implications for engagement and long-term retention.
Lower relapse rates. A study published in the Journal of Addictive Diseases found that participants in secular recovery programs had significantly lower rates of relapse compared to those attending traditional 12-step meetings, potentially attributable to the evidence-based, skill-building methods employed by secular programs.
Superior outcomes for co-occurring conditions. Brooks and Penn (2003), in a controlled study comparing 12-step and SMART Recovery approaches for individuals with co-occurring serious mental illness and substance use concerns (n=112), found that the cognitive-behavioral approach was more effective in improving health status, employment outcomes, and psychiatric stability. The 12-step approach was associated with worsening of medical problems and increased psychiatric hospitalization during follow-up.
More stable post-treatment mental health trajectories. Brown et al. (2006), in a randomized trial comparing 12-step facilitation with integrated cognitive behavioral treatment for veterans with co-occurring depression (n=66), found a significant divergence in post-treatment trajectories. CBT participants showed a steady linear decline in depression through six months post-treatment, while TSF participants’ depression scores initially improved during treatment but rebounded upward during the post-treatment follow-up period.
Stronger engagement among people with co-occurring conditions. Penn et al. (2016) conducted focus groups with clients (n=12) and counselors (n=7) experienced with both 12-step and SMART Recovery meetings. Both groups reported relatively more negative comments about 12-step programs, with concerns centering on the emphasis on powerlessness and spiritual concepts conflicting with therapeutic goals around self-efficacy and empowerment.
Research Summary
Across multiple studies and outcome measures, secular evidence-based programs demonstrate comparable abstinence rates, lower relapse rates, higher participant satisfaction among non-religious individuals, and superior outcomes for individuals with co-occurring mental health conditions. The body of evidence does not support characterizing these programs as lesser alternatives to 12-step models.
4. Comparative Analysis
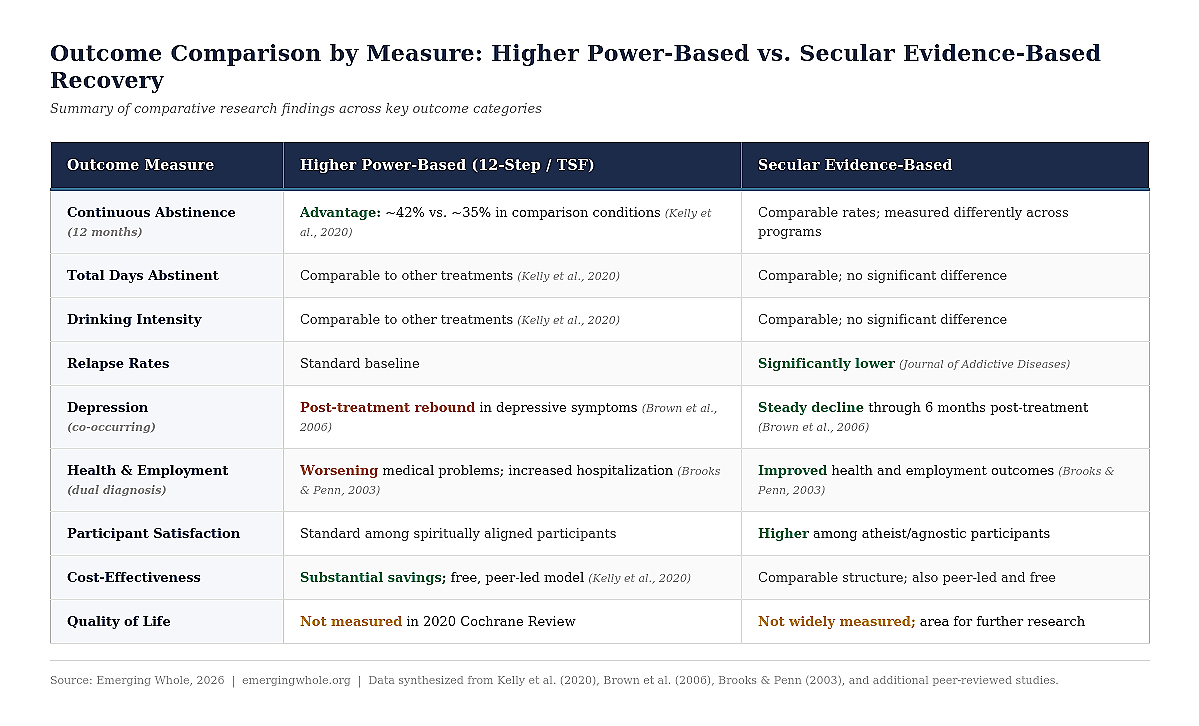
4.1 Outcome Comparison by Measure
The following table summarizes the comparative research findings across key outcome categories:
4.2 Support Structures: Sponsorship vs. Peer Facilitation
Beyond clinical outcomes, the two paradigms differ in how ongoing support is structured—a distinction with practical implications for safety and effectiveness, particularly for individuals with complex presentations.
The Sponsor Model
In 12-step programs, the sponsor relationship is a central support mechanism. A sponsor is a peer—not a therapist, counselor, or licensed professional—who has sustained personal recovery (typically one year or more) and has personally worked the 12 steps. Their role is to guide the sponsee through the same step-by-step process. Approximately 82% of 12-step participants engage with a sponsor, reflecting the centrality of this relationship within the model (Foy, 2026).
The strengths of this structure include personal accountability, the benefit of learning from someone with lived experience, and one-on-one availability. However, sponsors receive no formal training, licensing, or certification. They are not equipped to address complex mental health conditions, trauma responses, medication management, or co-occurring disorders. Their guidance is specific to the 12-step framework and rooted in personal experience rather than clinical training (Foy, 2026).
The Peer Facilitation Model
Secular programs generally employ a peer-facilitator model. Meetings are guided by trained facilitators or structured through group consensus, with emphasis on the group as a collaborative learning environment rather than a hierarchy of experience. Facilitators ensure that evidence-based tools are applied consistently, but do not serve as personal recovery authorities (Foy, 2026).
This structure prioritizes skill development and self-reliance. Participants acquire cognitive-behavioral strategies and rational thinking techniques designed for independent application, reducing dependence on any single individual for ongoing recovery management.
Structural Implication
For individuals with co-occurring mental health conditions—a substantial portion of the recovery-seeking population—the distinction between untrained peer sponsors and facilitated, evidence-based group models carries meaningful clinical relevance. The peer facilitation model may provide a more appropriate structure when complex conditions are present.
5. Implications and Recommendations
The evidence reviewed in this paper supports a clear conclusion: multiple recovery pathways are supported by research, and no single model demonstrates universal superiority across all outcome measures and population subgroups. This finding has practical implications for three key audiences.
5.1 For Clinicians and Treatment Providers
Referral practices should reflect the full evidence base. When 12-step programming is the default or sole recommendation, clinicians may inadvertently narrow recovery options for individuals better served by secular, evidence-based approaches—particularly those with co-occurring mental health conditions, those who identify as non-religious, have experienced religious trauma, or those who have previously disengaged from 12-step programs. The 2020 Cochrane Review itself acknowledged that secular mutual help organizations would presumably share the same cost-effectiveness benefits as 12-step groups (Heather, 2021). Clinicians are encouraged to present multiple options and support informed choice.
5.2 For Policymakers and Institutions
Court-mandated attendance at 12-step meetings—a common practice in many jurisdictions—warrants re-examination. The 2020 Cochrane Review explicitly excluded studies involving coerced participants, meaning its positive findings for AA/TSF cannot be applied to mandated treatment contexts. Policy should ensure that individuals in the justice system and publicly funded programs have meaningful access to multiple evidence-supported recovery models. Secular options should be funded and promoted with the same institutional support currently extended to 12-step programming.
5.3 For Individuals Seeking Recovery
The most effective recovery program is the one that aligns with the individual’s beliefs, needs, and clinical profile—and that the individual will actually engage with over time. Research consistently demonstrates that belief alignment with one’s primary support group is positively associated with active participation and improved outcomes. Individuals benefit from knowing that evidence-based secular options exist, are research-supported, and are available alongside traditional models. The decision between sponsorship and facilitated peer support, between spiritual and cognitive-behavioral frameworks, is personal—and the recovery system should support that choice rather than constrain it (Foy, 2026).
6. Areas for Further Research
Despite the growing evidence base, several significant gaps remain in the comparative literature:
Quality of life and psychological well-being. The 2020 Cochrane Review included no measures of quality of life—widely considered the ultimate aim of treatment. Future research should incorporate validated well-being instruments alongside abstinence and consumption metrics.
Long-term outcomes beyond abstinence. Both paradigms would benefit from longitudinal studies measuring identity reconstruction, relationship quality, employment stability, and life satisfaction—the outcomes that constitute sustained recovery, not merely sustained sobriety.
International and cross-cultural research. The vast majority of rigorous AA/TSF research has been conducted in the United States. The effectiveness and cultural adaptability of both secular and spiritual models in non-Western contexts requires dedicated investigation.
Real-world effectiveness vs. manualized protocols. Research on 12-step models has primarily evaluated clinically delivered, manualized TSF—not the typical peer-led, non-manualized experience most participants encounter. Studies measuring outcomes as people actually experience recovery support would substantially improve practical relevance.
Integrated and sequential approaches. Many individuals combine elements from multiple recovery models over time. Research on how integrated or sequential use of different frameworks affects long-term outcomes could inform more flexible, person-centered treatment planning.
7. Conclusion
The evidence reviewed in this paper demonstrates that higher power-based and secular recovery models each occupy a legitimate, research-supported position in the recovery landscape. The 12-step model’s strengths—community infrastructure, accessibility, structured progression, and decades of cultural presence—are well-documented. The secular model’s strengths—evidence-based tools, self-empowerment, adaptability for co-occurring conditions, and inclusivity across belief systems—are equally supported by peer-reviewed research.
The challenge facing the field is not a lack of evidence for multiple approaches. It is a lack of parity—in visibility, in institutional access, in referral practices, and in the assumptions that guide treatment decisions. When the research supports multiple pathways, the systems that serve people in recovery should reflect that.
Expanding the recovery landscape is not a zero-sum proposition. It does not diminish any single model. It strengthens the overall system by ensuring that more individuals find a pathway they can commit to, engage with consistently, and sustain over the long term—which is, ultimately, what the evidence tells us matters most.
References
Brooks, A. J., & Penn, P. E. (2003). Comparing treatments for dual diagnosis: Twelve-step and self-management and recovery training. The American Journal of Drug and Alcohol Abuse, 29(2), 359–383. https://doi.org/10.1081/ADA-120020519
Brown, S. A., Glasner-Edwards, S. V., Tate, S. R., McQuaid, J. R., Chalekian, J., & Granholm, E. (2006). Integrated cognitive behavioral therapy versus twelve-step facilitation therapy for substance-dependent adults with depressive disorders. Journal of Psychoactive Drugs, 38(4), 449–460. https://doi.org/10.1080/02791072.2006.10400584
Ferri, M., Amato, L., & Davoli, M. (2006). Alcoholics Anonymous and other 12-step programmes for alcohol dependence. Cochrane Database of Systematic Reviews, 2006(3). https://doi.org/10.1002/14651858.CD005032.pub2
Foy, C. (2026, January 26). What is a recovery sponsor and do you need one? FHE Health. https://fherehab.com/learning/recovery-sponsorship
Heather, N. (2021). Let’s not turn back the clock: Comments on Kelly et al. Alcohol and Alcoholism, 56(4), 377–379. https://doi.org/10.1093/alcalc/agaa137
Kelly, J. F., Humphreys, K., & Ferri, M. (2020). Alcoholics Anonymous and other 12-step programs for alcohol use disorder. Cochrane Database of Systematic Reviews, 2020(3). https://doi.org/10.1002/14651858.CD012880.pub2
Kelly, J. F., Abry, A., Ferri, M., & Humphreys, K. (2020). Alcoholics Anonymous and 12-step facilitation treatments for alcohol use disorder: A distillation of a 2020 Cochrane review for clinicians and policy makers. Alcohol and Alcoholism, 55(6), 641–651. https://doi.org/10.1093/alcalc/agaa050
Penn, P. E., Brooke, D., Brooks, A. J., Gallagher, S. M., & Barnard, A. D. (2016). Co-occurring conditions clients and counselors compare 12-step and SMART Recovery mutual help. Journal of Groups in Addiction & Recovery, 11(2), 76–92. https://doi.org/10.1080/1556035X.2015.1034824
Roth, J., White, W., & Kelly, J. (Eds.). Broadening the base of addiction mutual support groups: Bringing theory and science to contemporary trends. Routledge.
© 2026 Emerging Whole • emergingwhole.org