Beyond Abstinence
How Continuous Learning and Personal Growth Prevent Relapse and Sustain Long-Term Recovery
Executive Summary
Recovery from substance use or maladaptive behavior is not a single event but an ongoing process of growth, adaptation, and self-discovery. While significant attention and resources are devoted to achieving initial abstinence, research increasingly demonstrates that sustained recovery depends on what happens after that first milestone. Approximately 50% of individuals relapse within the first 12 weeks following intensive treatment (Guenzel & McChargue, 2023), a statistic that underscores a fundamental gap in how recovery is currently approached.
This white paper examines the evidence base for relapse prevention and makes the case that continuous learning, skill development, and intentional personal growth are not supplementary to recovery—they are central to it. Drawing on research in cognitive-behavioral therapy, continuing care models, and neuroplasticity, this paper argues that the most effective relapse prevention strategy is one that shifts focus from merely avoiding substances or behaviors to actively building a life worth sustaining.
The implications are significant for individuals in recovery, those who support them, and providers who serve them: recovery must be understood as a developmental process in which the capacity for growth is itself the most powerful protective factor against relapse.
The Relapse Problem: Why Abstinence Alone Is Not Enough
Relapse rates across substance use and behavioral recovery remain persistently high. Research has documented relapse rates of approximately 50% within the first 12 weeks after completion of intensive inpatient programs, many of which last 4 to 12 weeks and cost tens of thousands of dollars (Guenzel & McChargue, 2023). Despite the wide range of services available, no standardized relapse prevention programs have been established, and participation in interventions outside of the criminal justice system remains voluntary, making effectiveness difficult to measure.
These numbers do not represent moral failure. They represent a systems-level gap between what treatment typically provides and what sustained recovery actually requires.
Understanding Relapse as a Process
Clinicians and researchers have long recognized that relapse is a process, not an event. Guenzel and McChargue (2023) describe three distinct stages, each with identifiable signs and intervention opportunities:
Emotional relapse occurs when a person is not consciously thinking about using, but their emotions and behaviors—isolation, poor self-care, disrupted sleep, avoidance—are laying the groundwork for vulnerability. The individual may be in denial about their risk, which prevents them from using effective prevention techniques.
Mental relapse involves an internal tug-of-war between the desire to return to old patterns and the commitment to stay the course. Signs include romanticizing past use, minimizing consequences, bargaining, and actively planning opportunities to use.
Physical relapse is the final stage—the actual resumption of the substance or behavior. Critically, many physical relapses occur when the individual believes their use will go undetected, highlighting the role environment and accountability play in prevention.
"Consumption is the very last step in the relapse, and neglecting earlier events in a relapse prevents more effective intervention at earlier stages." — Guenzel & McChargue, 2023
This staged model reveals something important: the roots of relapse are emotional and cognitive long before they become behavioral. This means that effective prevention must also be emotional and cognitive—it must address how people think, feel, and cope, not merely whether they abstain.
The Stages of Recovery: A Developmental Lens
Research identifies three broad stages of recovery, each with distinct challenges and growth needs (Guenzel & McChargue, 2023):
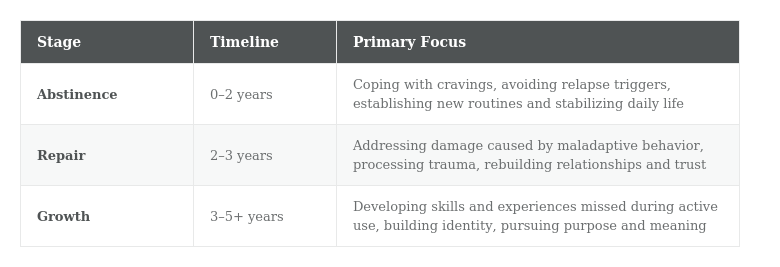
This framework illustrates that the work of recovery fundamentally changes over time. A person in the abstinence stage needs crisis-level coping tools. A person in the repair stage needs frameworks for processing pain and rebuilding trust. A person in the growth stage needs opportunities for purpose, skill-building, and identity development. No single intervention is adequate across all three stages—which is precisely why continuous learning matters.
The Evidence for Continuous Engagement
A growing body of research supports the principle that ongoing, adaptive engagement—not a single episode of treatment—is what drives long-term recovery outcomes.
Continuing Care and Long-Term Outcomes
McKay (2021) conducted an extensive review of continuing care research and found that, while individual study effects are sometimes small, the overall evidence supports a clear pattern: continuing care interventions of longer duration that include active efforts to keep individuals engaged produce more consistently positive results. A meta-analysis of 19 randomized trials found a statistically significant benefit for continuing care on substance use outcomes both at the end of interventions (Hedges’ g = 0.19) and at post-treatment follow-up (g = 0.27).
Critically, McKay’s review found that individuals at higher risk for relapse—those with continued substance use early in treatment, poor social support, or low motivation—benefited most from sustained continuing care. This suggests that the people who most need ongoing support are often those least likely to receive it under current treatment models.
The Role of Cognitive-Behavioral Approaches
Cognitive-behavioral therapy (CBT) remains one of the most widely studied and effective approaches for relapse prevention. CBT helps individuals identify and restructure the thought patterns that perpetuate harmful behavior, develop concrete coping skills, and build self-efficacy for managing high-risk situations (Guenzel & McChargue, 2023).
What makes CBT particularly relevant to a continuous learning model is its inherent structure: it teaches people how to think about their thinking. This is not a skill that is mastered once and set aside. It is a practice that deepens with time and application. Research on mindfulness-based relapse prevention (MBRP), which combines mindfulness practices with CBT principles, has shown that this integrated approach produces fewer days of substance use and heavy use at 12-month follow-up compared to traditional relapse prevention alone (McKay, 2021).
Technology-Supported Continuous Engagement
Emerging research on mobile health technology demonstrates that continuous, low-intensity support can meaningfully improve outcomes. In a controlled trial of the A-CHESS smartphone program, individuals with alcohol use disorder who had completed residential treatment reported significantly fewer risky drinking days and higher abstinence rates at 8- and 12-month follow-ups compared to those receiving standard care alone (McKay, 2021). Participants used the system on approximately 40% of the days they had access to it, suggesting that when accessible, ongoing support tools are available, people use them.
Similarly, a text-based recovery support program for youth (ESQYIR) found that those receiving daily recovery-oriented text messages were significantly less likely to test positive for their primary substance at 6- and 9-month follow-ups, and reported higher self-efficacy. The positive effects were mediated by increased involvement in pro-recovery activities, not merely by abstinence monitoring (McKay, 2021).
These findings point to a consistent theme: maintaining engagement in recovery-supportive learning and activity over time is itself a protective factor.
Growth as Relapse Prevention: A Framework
If relapse is a process that begins in emotional and cognitive territory, then prevention must also live in that territory. The most durable relapse prevention is not a set of avoidance strategies but a sustained commitment to building the internal resources—self-awareness, emotional regulation, cognitive flexibility, purpose, and connection—that make returning to old patterns less necessary and less appealing.
Neuroplasticity: The Brain’s Capacity for Change
The neuroscience of recovery provides a compelling biological basis for the continuous learning model. Sustained abstinence allows time for the brain to resume normal functioning, which can lay the foundations for long-term success (Guenzel & McChargue, 2023). Neuroplasticity—the brain’s ability to form new neural pathways—means that learning new skills, practicing new thought patterns, and engaging in new behaviors physically rewires the brain over time.
This is not metaphor. Every time a person practices a new coping strategy, challenges an automatic negative thought, or chooses a values-aligned action over an impulsive one, they are strengthening neural pathways that support recovery. The implication is clear: growth-oriented activity is not an add-on to recovery—it is the mechanism by which recovery becomes durable.
Five Domains of Continuous Growth
Drawing from the research, we identify five interconnected domains in which continuous learning serves as active relapse prevention:
1. Cognitive Skill Development
CBT, REBT, and related approaches teach individuals to identify irrational beliefs, challenge automatic negative thoughts, and develop more balanced thinking patterns. These are not static skills. As life circumstances change—new relationships, career challenges, grief, success—cognitive skills must be applied to new contexts. Ongoing practice and learning keep these tools sharp.
2. Emotional Regulation
Maladaptive behaviors often serve as emotional regulation strategies. When substances or behaviors are removed, the underlying emotional needs remain. Research on mindfulness-based approaches shows that developing a more nuanced relationship with one’s emotional life—rather than simply suppressing or avoiding difficult feelings—leads to better long-term outcomes. This is a lifelong learning process.
3. Relational Intelligence
Recovery fundamentally changes relationship dynamics. Rebuilding trust, setting boundaries, learning new communication patterns, and discerning which relationships to repair and which to release are complex interpersonal skills that develop over time with practice and reflection. Research on community reinforcement approaches, including CRAFT (Community Reinforcement and Family Training), demonstrates that involving supportive individuals in the recovery process improves outcomes (Guenzel & McChargue, 2023).
4. Identity Reconstruction
For many people, maladaptive behavior becomes intertwined with identity—particularly when the behavior began at a young age. Recovery requires constructing a new sense of self: clarifying values, identifying strengths, discovering interests, and building a narrative that integrates the past without being defined by it. This is not a one-time exercise but an evolving process that deepens over years.
5. Purpose and Meaning
McKay (2021) notes that effective continuing care must include provisions to promote greater involvement in “rewarding activities that provide enjoyment and a sense of meaning and purpose.” This finding aligns with a broad body of psychological research suggesting that a sense of purpose is protective against a wide range of mental health challenges, including relapse. Actively pursuing purpose—through work, service, creativity, education, or relationships—provides the forward momentum that sustains recovery over the long term.
Recovery is not the absence of a problem. It is the presence of growth—continuous, intentional, and deeply personal.
Bridging the Gap: From Treatment to Sustained Recovery
The current treatment landscape is structured around episodes of care: inpatient treatment, intensive outpatient programs, and aftercare referrals. While these interventions are critical, the research reveals a significant gap between the end of formal treatment and the long-term support needed to sustain recovery.
The Continuing Care Gap
McKay’s (2021) review identifies several challenges in the continuing care phase, including high dropout rates and the evolving clinical needs of individuals over time. Effective continuing care, he argues, must include elements that facilitate better retention and must be flexible enough to adapt to changing needs. Recovery management checkups (RMC), which provide assessments every three months with active reengagement when needed, have consistently produced better outcomes than assessment-only approaches—including more days of abstinence and fewer substance-related problems over multi-year follow-ups.
Yet much of the infrastructure for this kind of adaptive, long-term support remains inaccessible to the average person in recovery. This creates a gap that many individuals experience as a disorienting void: the intensive support of treatment ends, and they are left to navigate the complex work of rebuilding their lives with limited ongoing guidance.
What Effective Ongoing Support Looks Like
Research points to several characteristics of effective continuing care that can inform how we design recovery support systems:
• Longer duration: Interventions lasting 12 months or more produce more consistently positive results than shorter programs (McKay, 2021).
• Active engagement: Programs that include proactive outreach—not just passive availability—show stronger retention and outcomes.
• Adaptive design: The ability to adjust support based on an individual’s changing needs over time is critical. A one-size-fits-all approach fails to account for the reality that recovery is not linear.
• Skill-building focus: Approaches that teach transferable cognitive and emotional skills—rather than relying solely on monitoring or deterrence—equip people for the unpredictable challenges of real life.
• Connection to meaning: Recovery support that helps individuals engage in rewarding activities, community involvement, and purpose-driven pursuits shows the strongest long-term protective effects.
Implications and Recommendations
For Individuals in Recovery
Recovery is not something that happens to you—it is something you actively build. The research makes clear that ongoing engagement in learning, skill development, and personal growth is among the most powerful protections against relapse. This does not mean that relapse represents failure; the staged model of relapse shows that it is a process with identifiable warning signs and multiple intervention points. What it does mean is that recovery thrives when it is treated as a living, evolving practice rather than a static achievement.
Practical steps include seeking out educational resources on cognitive and emotional skills, maintaining connections with supportive communities, regularly reassessing personal values and goals, and actively pursuing activities that provide meaning and satisfaction.
For Providers and Treatment Systems
The evidence supports a shift from episodic treatment models to developmental recovery models that accommodate the changing needs of individuals over months and years. Providers should consider incorporating longer-duration continuing care plans, leveraging technology for between-session support, building assessment checkpoints into recovery plans, and emphasizing skill acquisition and personal development alongside abstinence maintenance.
As McKay (2021) notes, the field is moving toward evidence-based quality indicators for continuing care, including relapse prevention education, family involvement, a minimum of three months of follow-up, and patient involvement in developing their own care plans. These standards, when widely adopted, could meaningfully reduce the gap between treatment and sustained recovery.
For Community and Peer Support
Peer support plays an important but sometimes underexamined role in recovery. While evidence for the superiority of peer support groups over other interventions is limited, the social connection, accountability, and shared understanding they provide are difficult to replicate in clinical settings alone (Guenzel & McChargue, 2023). Peer support is most effective when it is grounded in evidence-based principles, adapted to individual needs, and focused on forward movement rather than solely on the past.
Conclusion
The research on relapse prevention tells a clear story: achieving abstinence is necessary, but it is not sufficient. Sustained recovery is built through continuous learning, adaptive coping, and intentional personal growth—over months, years, and a lifetime.
The three stages of recovery—abstinence, repair, and growth—each demand different skills, different support, and different kinds of learning. Relapse prevention is most effective when it meets people where they are in this developmental process and equips them not just to avoid old patterns, but to build new ones.
The brain’s capacity for change, the evidence for continuing care, and the protective power of purpose and meaning all point to the same conclusion: recovery is an active, ongoing process of becoming. The most important question is not “How do I avoid relapse?” but rather “What am I growing toward?”
When people have a compelling answer to that second question—supported by skills, community, and a commitment to continuous growth—relapse prevention becomes not a set of restrictions but a natural consequence of a life being well-lived.
References
Guenzel, N., & McChargue, D. (2023). Addiction relapse prevention. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK551500/
McKay, J. R. (2021). Impact of continuing care on recovery from substance use disorder. Alcohol Research: Current Reviews, 41(1), 01. https://doi.org/10.35946/arcr.v41.1.01
Witkiewitz, K., & Marlatt, G. A. (2004). Relapse prevention for alcohol and drug problems: That was Zen, this is Tao. American Psychologist, 59(4), 224–235. https://doi.org/10.1037/0003-066X.59.4.224