Understanding the Biopsychosocial Model
Why Biology, Psychology, and Social Environment All Matter in Recovery from Substance and Maladaptive Behavior
A comprehensive, evidence-based exploration of how biological predisposition, psychological experience, and social environment interact to shape both vulnerability and the path toward lasting recovery.
Executive Summary
For decades, the question of what causes compulsive substance use and maladaptive behavior has driven both scientific inquiry and public debate. Early models placed blame squarely on individual character, framing compulsive behavior as a moral failing. While the disease model that followed represented a significant step forward by legitimizing these conditions as medical concerns, it too offered an incomplete picture. Neither moral judgment nor biology alone can explain why one person develops a compulsive pattern while another, exposed to the same substance or behavior, does not.
The biopsychosocial model, first proposed by George Engel in 1977 and adapted for understanding substance use and maladaptive behavior by Marlatt and Baer in 1988, provides the most comprehensive framework available. It recognizes that a constellation of biological, psychological, and social factors converge to create each individual’s unique relationship with substances and behaviors. More importantly for those in recovery, this model illuminates why healing must address all three dimensions—not just the substance or behavior itself—to build a life that lasts.
“The bottom line is that there are likely as many pathways to becoming dependent on a substance as there are people who develop that dependence.”
This white paper examines the current evidence supporting the biopsychosocial model and translates these findings into practical understanding for individuals navigating recovery. The goal is not to reduce complex science to oversimplified takeaways, but to provide a grounded, accessible overview that empowers readers to understand why they respond the way they do—and what they can do about it.
1. Beyond Moral Failure: The Evolution of How We Understand Compulsive Behavior
The history of how societies have understood compulsive substance use and maladaptive behavior is, in many ways, a history of blame. For centuries, the prevailing belief was straightforward: people who used substances compulsively were morally weak. They lacked willpower. They made bad choices. This framing carried enormous consequences—it justified punishment over treatment, shame over support, and isolation over connection.
The moral model began to lose scientific credibility in the mid-twentieth century. In 1956, the American Medical Association declared alcoholism a disease requiring medical and psychological intervention (Mann et al., 2000). This was a watershed moment. It shifted the conversation from blame to biology and opened the door for research into the neurological underpinnings of compulsive behavior.
The disease model, sometimes referred to as the brain disease model, has been instrumental in reducing stigma and increasing access to treatment. However, it has also drawn criticism for being reductive. Framing compulsive behavior solely as a brain malfunction can undermine the complexity involved in its development and can inadvertently suggest that people lack agency in their own recovery (Borrell-Carrió et al., 2004). Researchers have increasingly argued for a more nuanced understanding—one that accounts for the full spectrum of human experience.
This is where the biopsychosocial model enters the conversation. Originally developed by psychiatrist George Engel as a framework for all medical practice, it was adapted to the study of compulsive substance use and behavior in the late 1980s. Rather than searching for a single cause, this model acknowledges that biological predisposition, psychological composition, and social environment all interact dynamically. Each person’s path toward compulsive behavior—and each person’s path toward recovery—is unique (Duncan, 2020).
Why This Matters for Recovery
Understanding the evolution of these models is not merely academic. The framework through which you understand your own experience shapes how you approach recovery. If you believe your struggles are a moral failing, you’ll carry shame. If you believe they’re purely biological, you may feel powerless. The biopsychosocial model offers something different: a framework that validates the complexity of your experience while simultaneously empowering you to address it from multiple angles.
2. The Biological Dimension: What Your Body Brought to the Table
Biology is a significant piece of the puzzle—but it is not the entire puzzle. While no single gene determines whether someone will develop compulsive substance use or maladaptive behavior, decades of research through twin studies, adoption studies, family studies, and epigenetic research have established that these conditions carry a heritable component. The estimated heritability for substance use disorders ranges from 40–60%, depending on the specific substance (Giordano, 2021).
The Reward System and Dopamine
At the neurological level, all substances and behaviors that carry potential for compulsive use share a common mechanism: they activate the brain’s dopamine-driven reward system. The mesolimbic pathway—the circuit connecting the ventral tegmental area to the nucleus accumbens—is designed to reinforce behaviors essential for survival: eating, bonding, and reproducing. Substances of abuse co-opt this system, typically producing dopamine surges that far exceed what natural rewards generate.
What makes this especially relevant is that the intensity of this reward experience varies significantly from person to person. One hypothesis, known as Reward Deficiency Syndrome, proposes that some individuals are born with underactive reward circuitry (Blum et al., 2014). These individuals may experience baseline states of restlessness, dissatisfaction, or emotional flatness that make the rewarding effects of substances or behaviors particularly powerful—not because they lack willpower, but because their neurochemistry is wired differently.
Multiple neurotransmitter systems are involved beyond dopamine alone, including opioid peptides, GABA, serotonin, endocannabinoids, and glutamate (Blum et al., 2020). Deficiencies or dysregulation in any combination of these neurochemicals may contribute to vulnerability. This biological variability is one reason why empathy is so critical in recovery spaces: it is very likely that two people experience the same substance in fundamentally different ways.
Neuroplasticity: The Brain Can Heal
Perhaps the most hopeful finding from neuroscience research is the concept of neuroplasticity—the brain’s ability to reorganize itself by forming new neural connections throughout life. While substance use and maladaptive behavior create powerful neural pathways that reinforce compulsive patterns, these pathways are not permanent. With sustained abstinence, therapeutic intervention, and the development of new behavioral patterns, the brain can and does rewire itself (Andrew Bickel, 2024).
Research demonstrates that the prefrontal cortex—the brain region responsible for judgment, planning, and impulse control—can regain function during recovery. Activities such as mindfulness practice, physical exercise, cognitive behavioral therapy, and the development of meaningful social connections all stimulate neuroplastic change. Exercise, for example, has been shown to promote dopamine regulation, increase serotonin availability, and support the release of neurotrophic factors that encourage neural growth and repair (Tomczyk et al., 2024).
Your brain adapted to compulsive patterns through repetition. It can adapt to healthy patterns the same way. Neuroplasticity is the biological basis for the belief that change is always possible.
3. The Psychological Dimension: What Your Mind Was Trying to Solve
The psychological dimension of the biopsychosocial model encompasses personality traits, mental health conditions, cognitive patterns, self-concept, and the cumulative impact of life experiences—particularly trauma. This dimension addresses a question that the biological model alone cannot answer: why does a person start using a substance or engaging in a behavior in a way that becomes compulsive?
For many people, the answer involves emotional regulation. Substances and maladaptive behaviors often serve a purpose. They manage anxiety. They numb pain. They create a sense of control in environments that feel chaotic. They provide temporary relief from depression, hypervigilance, or feelings of worthlessness. Understanding this function is not making excuses—it is acknowledging that human beings are wired to seek relief from suffering, and sometimes the tools available are harmful ones.
Adverse Childhood Experiences and Trauma
The connection between early adversity and later compulsive behavior is among the most robust findings in the field. The original Adverse Childhood Experiences (ACEs) study conducted by Felitti and colleagues (1998) established a clear dose-response relationship: the more categories of childhood adversity a person experienced, the greater their risk for substance use and a range of other health outcomes.
Recent research has continued to strengthen these findings. A 2023 longitudinal study following over 8,000 participants found that adults with any history of ACEs had a 4.3-fold higher likelihood of developing a substance use disorder. The associations were gender-specific: women showed a 5.9-fold increase in alcohol use disorders, while men showed a 5.0-fold increase in illicit drug use disorders (Kvestad et al., 2023). Data from the CDC’s 2023 Youth Risk Behavior Survey found that three in four high school students reported experiencing at least one ACE, and that preventing ACEs could reduce prescription pain medication misuse by as much as 84% (Swedo et al., 2024).
The mechanism connecting trauma to compulsive behavior involves the stress response system. Chronic exposure to adversity during development can dysregulate the hypothalamic-pituitary-adrenal (HPA) axis, leading to chronically elevated cortisol and adrenaline. Individuals living in this state of persistent hyperarousal and hypervigilance may find that substances or behaviors offer the only reliable way to regulate their emotional experience (van der Kolk, 2014; Burke Harris, 2018).
Psychological Factors Beyond Trauma
While trauma is a significant contributor, the psychological dimension extends further. Personality traits such as sensation-seeking and impulsivity, co-occurring mental health conditions including anxiety and depression, and psychological constructs such as self-esteem and attachment style all influence vulnerability. Research has identified a bidirectional relationship between depression and substance use: individuals with ACEs are more likely to develop depression, and depression significantly increases the likelihood of using substances as a coping mechanism (Wu et al., 2022).
For recovery, this dimension carries a critical implication: addressing the substance or behavior alone is insufficient. If the underlying psychological needs that drove the compulsive pattern remain unaddressed—the unprocessed trauma, the untreated anxiety, the fractured sense of self—the risk of returning to old patterns remains high. Recovery must include the work of understanding what your mind was trying to solve.
4. The Social Dimension: The World You Lived In
The third dimension of the biopsychosocial model recognizes that individual behavior exists within a social context. No one develops compulsive patterns in a vacuum. Social norms, environmental availability, cultural messaging, economic conditions, community structure, and interpersonal relationships all shape the experience of substance use and maladaptive behavior.
Social Modeling and Norms
Social learning theory tells us that behavior is shaped significantly through observation. A child who grows up watching a parent use alcohol to manage stress absorbs a powerful, unspoken lesson about how adults cope with difficulty. Community-level norms—such as the widely held belief that experimentation with substances is a normal part of certain life stages—further normalize behavior that carries real risk for vulnerable individuals.
Availability, Access, and Targeting
Research consistently demonstrates that communities with greater availability and more aggressive marketing of substances experience higher rates of use. Impoverished communities are disproportionately targeted with alcohol and tobacco advertising and have more points of sale per capita than more affluent areas (Primack et al., 2007; Rose et al., 2019). This is not a matter of individual choice existing in isolation—it is a matter of individual choice existing within a system designed to influence it.
Social Environment and Recovery
The social dimension is equally critical during recovery. Research on recovery capital—the internal and external resources that support sustained recovery—has identified social connection as one of the strongest predictors of long-term success. A 2023 systematic review analyzing 69 studies found that recovery capital, conceptualized through a biopsychosocial framework, provides a measurable way to identify both strengths and barriers that can be targeted to support recovery (Thege et al., 2023).
The quality of relationships, the presence of a supportive community, stable housing, meaningful employment, and a sense of belonging all constitute social recovery capital. Conversely, isolation, returning to environments associated with past use, and relationships that lack healthy boundaries can undermine even the strongest biological and psychological recovery work.
Recovery does not happen in isolation. The social dimension reminds us that building a life worth living requires building a world worth living in—one relationship, one community, and one environment at a time.
5. Putting It All Together: An Integrated Model for Recovery
The power of the biopsychosocial model lies not in any single dimension, but in the interaction among all three. A person may carry a genetic predisposition (biological), experience childhood trauma that dysregulates their stress response (psychological), and grow up in a community where substance use is normalized and readily available (social). None of these factors alone is sufficient to predict compulsive behavior—but together, they create a constellation of risk that is greater than the sum of its parts.
The following table illustrates how each dimension contributes to both risk and recovery:
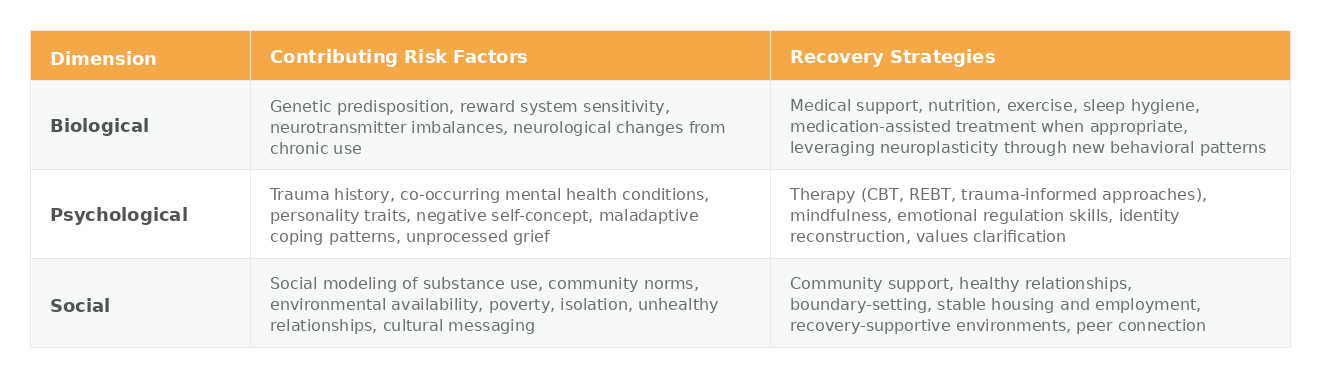
This integrated approach has significant implications for how we structure recovery support. Treatment that addresses only the biological dimension—detoxification and medication—may resolve the immediate physiological crisis but leave the psychological and social drivers intact. Therapy that addresses only the psychological dimension may build insight without addressing the neurological changes or environmental triggers. Community support that addresses only the social dimension may provide belonging without equipping individuals with the internal tools they need.
Effective recovery addresses all three dimensions, simultaneously and over time. This is not a linear process. It requires patience, flexibility, and a willingness to work on the dimension that is most pressing at any given stage. Early recovery may prioritize biological stabilization. Later stages may focus more heavily on psychological growth and social reconstruction. The biopsychosocial model provides a framework for understanding where you are and what you need—without judgment about where you should be.
6. Practical Applications: Using This Framework in Your Recovery
Understanding the biopsychosocial model is not just an intellectual exercise. It is a practical tool for building a recovery plan that addresses the full complexity of your experience. The following considerations can guide your approach:
Assess All Three Dimensions
Biological: What do you know about your family history? Have you discussed potential medication support with a healthcare provider? Are you attending to physical health fundamentals—nutrition, movement, sleep? These are not secondary concerns; they are foundational to the brain’s ability to heal.
Psychological: Have you explored the emotional needs that your substance or behavior was meeting? Are there unprocessed experiences that continue to drive your emotional responses? Working with a therapist trained in evidence-based approaches such as CBT, REBT, or trauma-informed modalities can help you develop new ways of meeting those needs.
Social: What does your social environment look like? Are you surrounded by people and contexts that support your recovery, or ones that undermine it? Building recovery capital in the social dimension may require difficult but necessary changes—setting boundaries, leaving certain environments, and intentionally cultivating new connections.
Resist Single-Cause Thinking
The biopsychosocial model challenges us to resist the temptation of simple explanations. Your experience was not caused by one thing, and it will not be resolved by one thing. Be wary of any approach—clinical, cultural, or personal—that claims a single answer. The research is clear: the most effective pathways to lasting recovery are multifaceted and holistic (Marlatt & Baer, 1988).
Practice Self-Compassion Informed by Science
Perhaps the most important practical takeaway from the biopsychosocial model is this: your experience of compulsive behavior was shaped by forces far more complex than personal weakness. Genetics you did not choose, experiences you may not have had the power to prevent, and environments you may not have been able to control all played a role. Understanding this is not about abdicating responsibility for your recovery—it is about approaching that responsibility with compassion rather than shame.
7. Conclusion: A Framework for Wholeness
The biopsychosocial model of substance use and maladaptive behavior represents the most comprehensive, evidence-based understanding available. It honors the complexity of the human experience by acknowledging that biology, psychology, and social environment are not competing explanations but interacting forces that shape both vulnerability and resilience.
For individuals in recovery, this framework offers both validation and direction. It validates the real, measurable biological changes that make compulsive behavior so persistent. It validates the psychological pain that often drives the initial turn toward substances or behaviors. It validates the social conditions that make some environments far more dangerous than others. And it directs attention toward a recovery approach that is as multifaceted as the challenge itself.
At Emerging Whole, we believe that sobriety is just the beginning. The biopsychosocial model reinforces this conviction. Getting free from a substance or behavior is the essential first step. Building a life that addresses the biological, psychological, and social dimensions of your experience—that is the longer, deeper, more rewarding work of becoming whole.
Recovery asks us to rebuild across every dimension of our lives. The biopsychosocial model is a map for that rebuilding—one that takes the full complexity of who you are seriously.
References
Andrew Bickel, M. (2024). Neuroplasticity and addiction: Understanding brain rewiring during substance use and recovery. Journal of Addiction Research & Therapy, 15, 729. https://doi.org/10.4172/2155-6105.100729
Blum, K., Thanos, P. K., & Gold, M. S. (2014). Dopamine and glucose, obesity, and reward deficiency syndrome. Frontiers in Psychology, 5, 919. https://doi.org/10.3389/fpsyg.2014.00919
Blum, K., Gondre-Lewis, M. C., Baron, D., Thanos, P. K., Braverman, E. R., Neary, J., Elman, I., & Badgaiyan, R. D. (2020). Introducing precision addiction management of reward deficiency syndrome, the construct that underpins all addictive behaviors. Frontiers in Psychiatry, 11, 548316. https://doi.org/10.3389/fpsyt.2020.548316
Borrell-Carrió, F., Suchman, A. L., & Epstein, R. M. (2004). The biopsychosocial model 25 years later: Principles, practice, and scientific inquiry. Annals of Family Medicine, 2(6), 576–582. https://doi.org/10.1370/afm.245
Burke Harris, N. (2018). The deepest well: Healing the long-term effects of childhood adversity. Houghton Mifflin Harcourt.
Duncan, P. M. (2020). Substance use disorders: A biopsychosocial perspective. Cambridge University Press.
Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196(4286), 129–136. https://doi.org/10.1126/science.847460
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Giordano, A. L. (2021, July 10). What exactly is the biopsychosocial model of addiction? Psychology Today. https://www.psychologytoday.com/us/blog/understanding-addiction/202107/what-exactly-is-the-biopsychosocial-model-addiction
Grisel, J. (2019). Never enough: The neuroscience and experience of addiction. Doubleday.
Kvestad, I., Heradstveit, O., Hysing, M., Nilsen, S. A., Øverland, S., & Boe, T. (2023). Adverse childhood experiences and their association with substance use disorders in adulthood: A general population study (Young-HUNT). Drug and Alcohol Dependence, 245, 109830. https://doi.org/10.1016/j.drugalcdep.2023.109830
Mann, K., Hermann, D., & Heinz, A. (2000). One hundred years of alcoholism: The twentieth century. Alcohol and Alcoholism, 35(1), 10–15. https://doi.org/10.1093/alcalc/35.1.10
Marlatt, G. A., & Baer, J. S. (1988). Addictive behaviors: Etiology and treatment. Annual Review of Psychology, 39, 223–252. https://doi.org/10.1146/annurev.ps.39.020188.001255
Primack, B. A., Bost, J. E., Land, S. R., & Fine, M. J. (2007). Volume of tobacco advertising in African American markets: Systematic review and meta-analysis. Public Health Reports, 122(5), 607–615. https://doi.org/10.1177/003335490712200508
Rose, S. W., Barker, D. C., D’Angelo, H., Khan, T., Huang, J., Chaloupka, F. J., & Ribisl, K. M. (2019). The availability of electronic cigarettes in U.S. retail outlets, 2012–2015. Tobacco Control, 28(3), 203–209. https://doi.org/10.1136/tobaccocontrol-2017-053789
Swedo, E. A., Pampati, S., Anderson, K. N., et al. (2024). Adverse childhood experiences and health conditions and risk behaviors among high school students — Youth Risk Behavior Survey, United States, 2023. MMWR Supplements, 73(Suppl-4), 39–49. https://doi.org/10.15585/mmwr.su7304a5
Thege, B. K., White, W. L., Gmös, A. F., et al. (2023). Measuring recovery capital for people recovering from alcohol and drug addiction: A systematic review. Addiction Research & Theory, 32(3), 225–236. https://doi.org/10.1080/16066359.2023.2245323
Tomczyk, S., Isensee, B., & Hanewinkel, R. (2024). Strengthening neuroplasticity in substance use recovery through lifestyle intervention. American Journal of Lifestyle Medicine, 18(5), 647–659. https://doi.org/10.1177/15598276241253590
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Viking.
Wu, Y., Zhang, L., Ai, M., Wang, J., & Kuang, L. (2022). Does childhood adversity lead to drug addiction in adulthood? A study of serial mediators based on resilience and depression. Frontiers in Psychiatry, 13, 871459. https://doi.org/10.3389/fpsyt.2022.871459